Psychology
Mar 21, 2026
Introduction to Psychology
Cognitive Psychology
Developmental Psychology
Abnormal Psychology
Social Psychology
Biopsychology/Neuroscience
Why Obesity Drug Equity Is Also a Psychology Story
A Lancet editorial argues 2026 could be a turning point for fairer access to GLP-1 obesity treatment. The deeper issue is not just patents or price, but how stigma, scarcity, and c
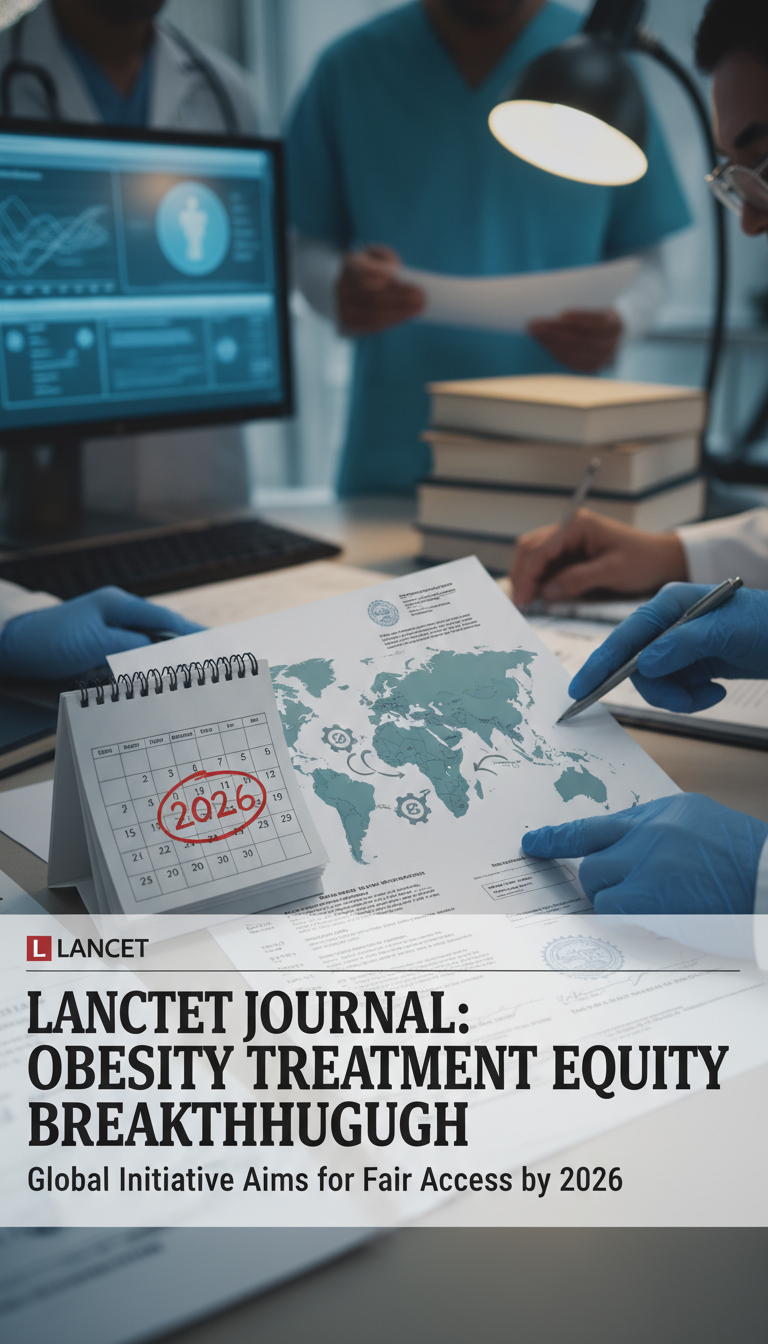
The Lancet’s new editorial on obesity treatment equity is getting attention for a practical reason: 2026 may be the year GLP-1 drugs become far more affordable in many countries. But the most important layer is psychological. Obesity is still widely treated as a character flaw rather than a chronic disease, and that belief changes who asks for help, who gets judged, who can stay on treatment, and who is blamed when weight returns.
If access expands without changing that mindset, cheaper drugs could still leave the most stigmatized patients behind. And if the public keeps seeing GLP-1s as either a miracle cure or a vanity shortcut, disappointment, shame, and black-market demand will keep growing.
Why this editorial matters now
The editorial’s headline claim is striking: as patents begin expiring in countries such as Brazil, China, and India, generic or biosimilar semaglutide could potentially be produced at very low cost, with estimates around $28 per person-year for injectable drug supply. That matters because obesity affects more than a billion people worldwide, with a large share of the burden in low- and middle-income countries.
It also highlights a less obvious barrier: delivery systems. Injectable pens can cost many times more than the drug itself, and companies can use dense patent strategies around devices to delay competition even when the core molecule is nearing wider availability.
Explore our free psychology courses
Introduction to Psychology
University · Psychology
Cognitive Psychology
University · Psychology

Developmental Psychology
University · Psychology
Abnormal Psychology
University · Psychology
Social Psychology
University · Psychology

Biopsychology/Neuroscience
University · Psychology
How stigma turns a medical problem into a psychological trap
Obesity stigma does more than hurt feelings. It changes behavior. People who expect judgment from clinicians often delay care, avoid weigh-ins, or drop out after a shaming encounter. That means the same social groups with the highest obesity burden can become the least likely to receive consistent treatment.
Scarcity makes this worse. When expensive drugs are seen on celebrities and wealthy patients first, the public story becomes moralized: disciplined elites versus irresponsible others. Psychologically, that reinforces shame rather than treatment-seeking. It also fuels resentment, which helps misinformation spread faster online.
So how could wider access reduce stigma rather than deepen it? By changing the frame. When treatment is visibly available through ordinary health systems, obesity looks less like a luxury self-improvement project and more like what it is: a chronic condition that deserves routine care. That does not erase bias overnight, but it weakens the idea that only the rich are “worthy” of medical help.
Why cheaper drugs still will not be enough
One major misconception is that GLP-1 drugs “cure” obesity. They can be highly effective, but many patients regain weight after stopping, often within about 18 months. That means obesity management is usually long-term, not a one-time fix.
This is where psychology becomes central. Adherence is not just remembering a dose. It involves expectations, side effects, cost anxiety, family pressure, stigma, depression, and the emotional impact of regain. If patients start treatment believing it will permanently solve everything, normal setbacks can feel like personal failure.

Better support usually includes:
- clear counseling that obesity is chronic and relapse risk is real
- behavioral support focused on routines, stress, and eating environments
- non-stigmatizing follow-up when weight loss slows or reverses
- practical planning for interruptions, shortages, or switching products
In other words, the drugs work through biology, but staying well depends heavily on psychology and environment.
What drives black markets and unsafe use
Weak evidence does not stop demand when a treatment becomes a status symbol. Black markets grow when three forces combine: high price, high hope, and high shame. People who feel judged in formal care may turn to unsupervised channels, especially if they believe needing help is embarrassing.
That is why regulation alone is not enough. Safer access requires trusted clinics, plain-language education, and messaging that separates medically supervised obesity treatment from aspirational “vanity” use. Otherwise, scarcity and stigma keep pushing vulnerable people toward counterfeit or inappropriate products.
What a fairer future would actually look like
The best-case scenario is not simply “everyone gets a GLP-1.” It is a system where lower-cost medicines, simpler delivery options, and primary-care access are combined with anti-stigma practice and healthier food environments. Oral GLP-1 options may help in places where refrigeration and injection logistics are difficult, but they still need follow-up and realistic counseling.
Equity will succeed only if policy answers two questions at once: can people obtain treatment, and can they do so without humiliation? If the answer to the second question is no, the first will never be enough.

Conclusion
So why won’t cheaper GLP-1s alone fix obesity inequity? Because the real barriers are also social and psychological: stigma, distrust, unrealistic expectations, and unequal care systems. And how could wider access reduce stigma instead of worsening it? By making obesity treatment ordinary, chronic-disease care rather than a luxury product for the already privileged. The 2026 shift could be historic, but only if access and dignity expand together.